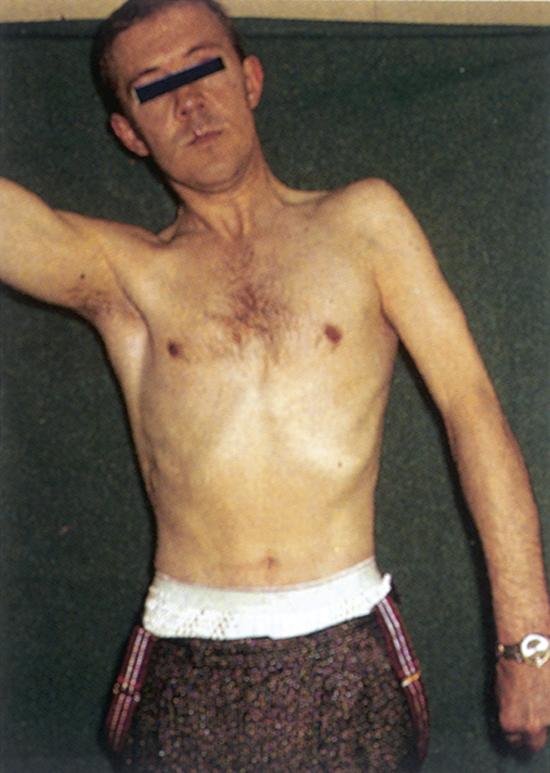
syringomyelia /-mī·ē″lyə/ [Gk, syrinx, tube, myelos, marrow] , a chronic progressive disease of the spinal cord, marked by elongated central fluid-containing cavities surrounded by gliosis or a proliferation of neurological tissue. Symptoms begin early in adulthood, usually involving the cervical region, with muscular wasting in the upper limbs. The disease is more common in males. ▪ OBSERVATIONS: Although present at birth, onset is insidious, and manifestations are often not seen until individuals are in their 20s or 30s. These symptoms are often ambiguous and mimic a host of other diseases. The cervical spine is most commonly affected and manifests as weakness, atrophy, and sensory loss in the shoulders, arms, and hands, including loss of pain and temperature sensation and sweating on the face. Upper extremity reflexes are diminished or absent, whereas weakness, altered gait, spasticity, and hyperreflexia may be noted in the lower extremities. Brainstem involvement may cause dysphagia, ptosis, miosis, or diplopia. GI symptoms include nausea, vomiting, weight loss, and abdominal spasms. Respiratory disturbances may manifest during sleep. Joint arthropathy and trophic skin changes may eventually develop. The course of the disease is variable and may result in slow, long-term incapacitation. Disease progress may slow or stop at any time. Diagnosis is made through MRI. Bony abnormalities at the base of the skull and C1-2 spine and scoliosis may be seen on x-ray. ▪ INTERVENTIONS: The primary intervention is a cervical decompression laminectomy at C1-2 spine with repair or removal of bony abnormalities, with possible myelotomy or shunt placement. Although surgical intervention halts disease progression, it seldom leads to significant improvement in current neurological manifestations. ▪ PATIENT CARE CONSIDERATIONS: Nursing care after surgery is aimed at careful positioning and turning to maintain proper alignment of the cervical spine and head; control of postoperative pain; surgical wound care; monitoring for CSF leakage and peripheral vital signs; assessment of motor and sensory function in the extremities and bowel and bladder function. Chronic care focuses on rehabilitation for the sequelae from neurological damage that occurred before the surgery. These are varied and may include bowel and bladder programs for management of neurogenic bowel or bladder; protection against injury and breakdown of skin related to decreased sensation; physical therapy to build strength and endurance; occupational therapy to improve or adapt functioning; respiratory therapy to increase vital capacity and tidal volume; and speech therapy if swallowing is affected. Counseling and support services are provided for the individual and family to aid in adaptation.