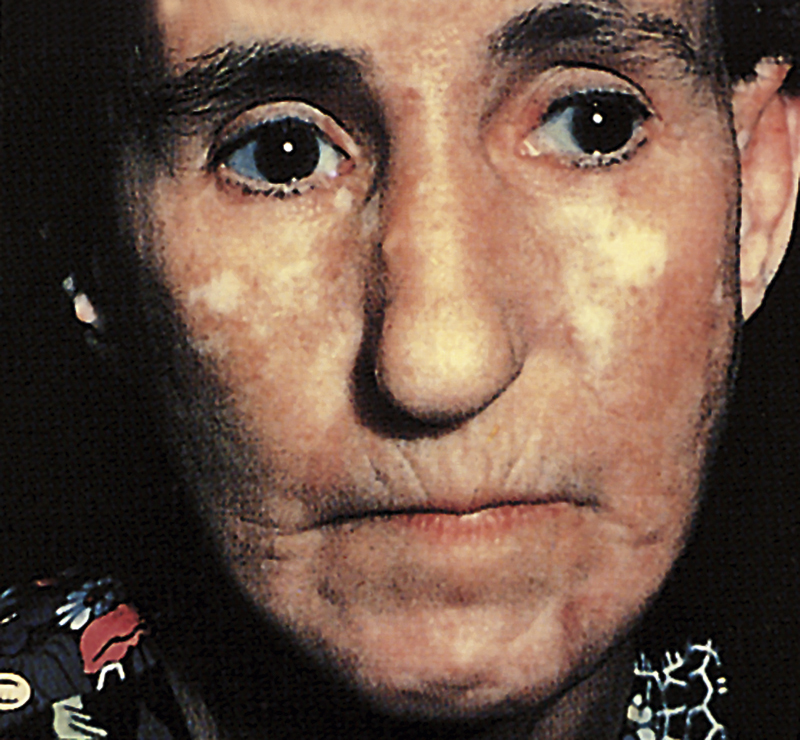
scleroderma /sklir′ōdur″mə/ [Gk, skleros + derma, skin] , chronic hardening and thickening of the skin caused by new collagen formation, with atrophy of pilosebaceous follicles. Scleroderma is most common in middle-aged women. It may occur in a localized form (morphea) or as a systemic disease (systemic sclerosis). Progressive systemic sclerosis (PSS) is a relatively rare autoimmune disease affecting the blood vessels and connective tissue. It is characterized by fibrous degeneration of the connective tissue of the skin, lungs, and internal organs, especially the esophagus, digestive tract, and kidneys. See also morphea, systemic sclerosis. ▪ OBSERVATIONS: The most common initial complaints are changes in the skin of the face and fingers. Raynaud’s phenomenon occurs with a gradual hardening of the skin and swelling of the distal extremities. In the early stages the disease may be confused with rheumatoid arthritis or Raynaud’s disease. As the disease progresses, deformity of the joints and pain on movement occur. Skin changes include edema and then pallor; then the skin becomes firm; finally it becomes slightly pigmented and fixed to the underlying tissues. At this stage the skin of the face is taut, shiny, and masklike, and the patient may have difficulty in chewing and swallowing. Patients with mild forms of scleroderma may live to 30 to 50 years of age. Those with cardiac, renal, pulmonary, or intestinal involvement may die at an earlier age. The usual indication that renal disease is present is the abrupt onset of severe arterial hypertension that does not respond to medication. Localized forms of scleroderma may occur; these cases are benign and appear only as small circumscribed patches on the skin. A biopsy of the lesion may be done to diagnose the condition. Radiographic examination of the lungs and GI tract may be diagnostic in the systemic form of the disease. Blood tests may reveal antinuclear antibodies. ▪ INTERVENTIONS: There are no drugs to cure scleroderma; however, corticosteroids, immunosuppressants, antacids, and histamine receptor antagonists may be useful in treating the symptoms of the disease, and salicylates and mild analgesics are given to ease pain in the joints. Physical therapy slows the development of muscle contracture and resultant deformity and debility. Nephrectomy or renal transplantation may be performed. ▪ PATIENT CARE CONSIDERATIONS: The health care provider advises patients to use mild, nonalcoholic astringent soaps; to avoid extreme cold and activities that trigger pain; to wear gloves; to stop smoking; and to eat small, frequent meals. In the advanced stages of scleroderma patients often require help to eat, and mouth and skin care is particularly important. As patients become more helpless, there is a need for considerable emotional support.