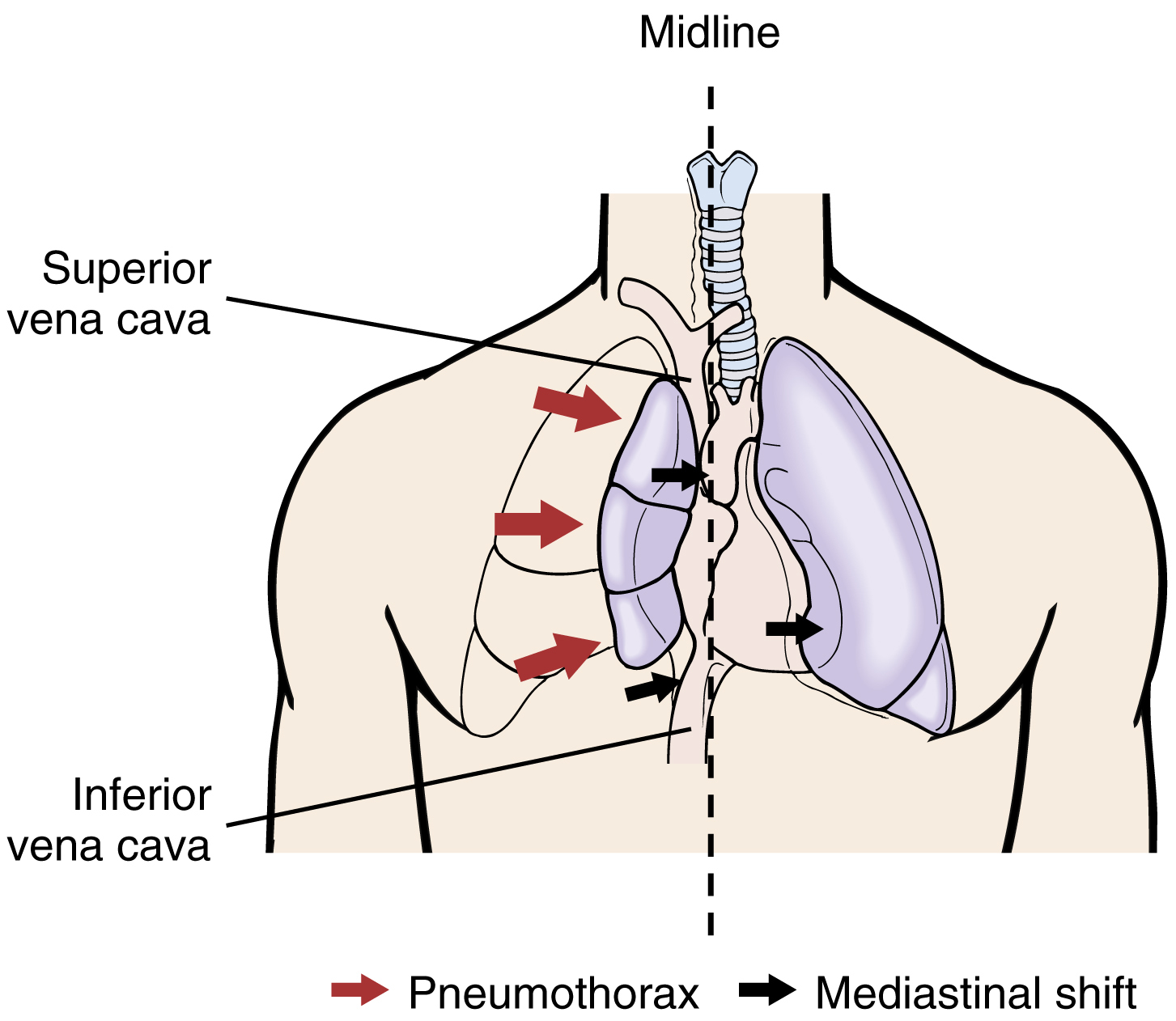
pneumothorax /no̅o̅′mōthôr″aks/ [Gk, pneuma, air, thorax, chest] , the presence of air or gas in the pleural space, causing a lung to collapse. Pneumothorax may be the result of an open chest wound that permits the entrance of air, the rupture of an emphysematous vesicle on the surface of the lung, or a severe bout of coughing. It may also occur spontaneously without apparent cause. ▪ OBSERVATIONS: The onset of pneumothorax is accompanied by a sudden sharp chest pain, followed by difficult, rapid breathing; decreased breath sounds and cessation of normal chest movements on the affected side; tachycardia; a weak pulse; hypotension; diaphoresis; an elevated temperature; pallor; dizziness; and anxiety. ▪ INTERVENTIONS: The patient is assured that the condition can be treated, is urged to remain still, and is placed in bed in Fowler’s position. Oxygen is administered through a nasal cannula, unless contraindicated, and the air in the pleural space is immediately aspirated. A chest tube is inserted and attached to an underwater seal; a waterless, disposable system; or a mobile chest drain; the tube is not removed until air is no longer expelled through the seal and a radiographic examination shows that the lung is completely expanded. Pain may be controlled by administering appropriate analgesics, but the use of respiratory depressants is avoided. Intermittent positive-pressure breathing may be administered. ▪ PATIENT CARE CONSIDERATIONS: The patient is taught how to turn, cough, breathe deeply, and perform passive exercises and is told to avoid stretching, reaching, or making sudden movements. The patient is advised not to smoke but to drink fluids copiously, to exercise, to avoid fatigue and strenuous activity, and to report any symptoms of recurrence, such as chest pain, difficult breathing, fever, or respiratory infection.