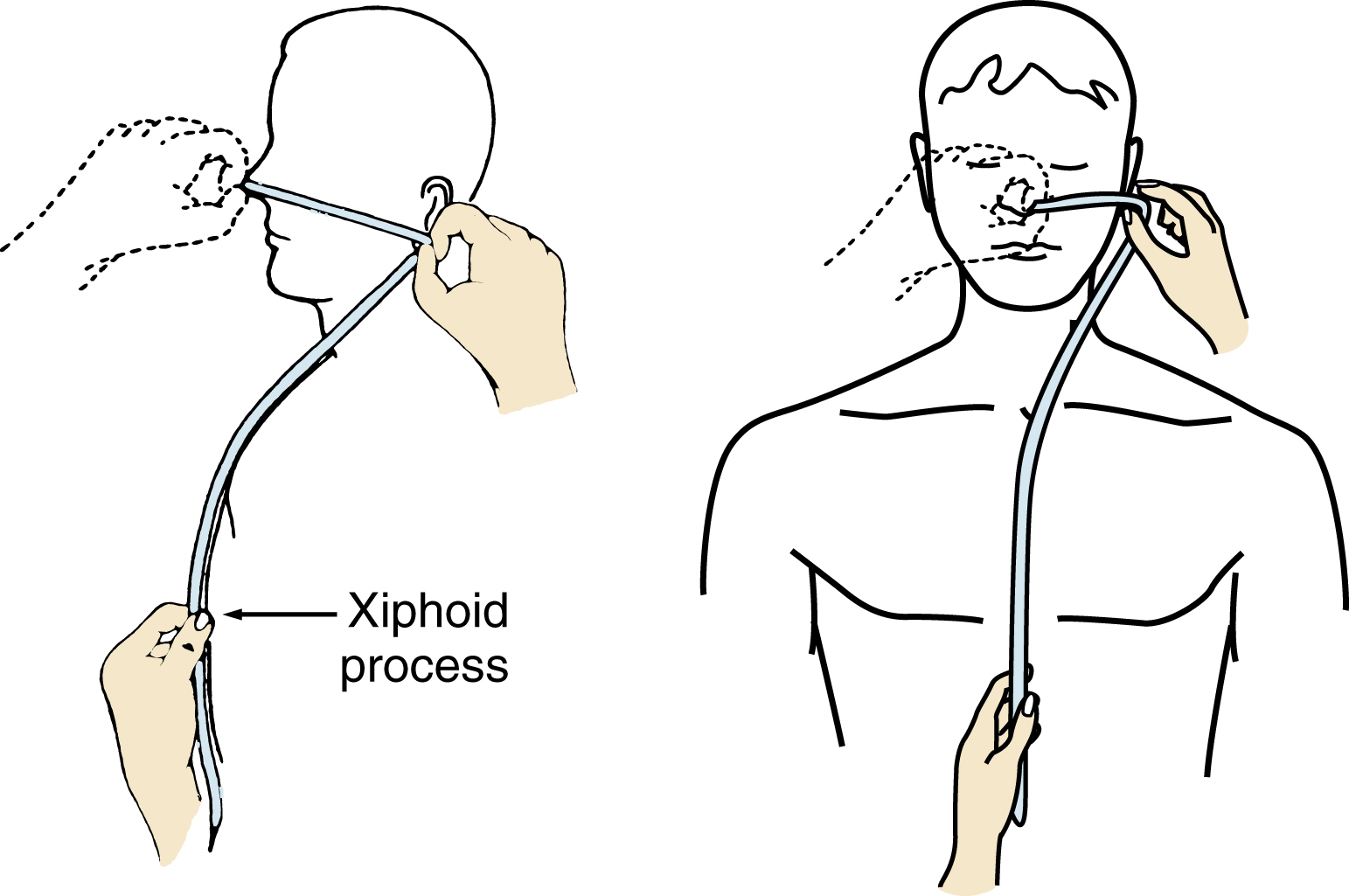
nasogastric intubation, the placement of a nasogastric tube through the nose into the stomach to relieve gastric distension by removing gas, gastric secretions, or food; to instill medication, food, or fluids; or to obtain a specimen for laboratory analysis. After surgery and in any condition in which the patient is able to digest food but not eat it, the tube may be introduced and left in place for tube feeding until the ability to eat normally is restored. ▪ METHOD: A French size 12 to 18 plastic or rubber catheter is selected. The procedure is explained to the patient. Nares are assessed for any obstructions, deformations, deformities, or tissue irritation. If the catheter is rubber, it is soaked in ice water to stiffen and lubricate it. The patient is placed in an upright sitting position, and a towel or bib is placed over the chest. The necessary length of tube is marked off; it is the same as the distance from the tip of the nose to the earlobe plus the distance to the xiphoid process. The tip of the tube may be lubricated with a water-soluble lubricating jelly, but, if a specimen is to be obtained for cytological study, water or saline solution is preferred. The tube is grasped and held 7.5 cm from the tip and is placed in the nostril, where it is advanced forward and downward. When it has been passed 7.5 cm, it is in the pharynx. The patient is then asked to bend the neck forward, to take shallow rapid breaths, and to help advance the tube by swallowing. If the patient is able to drink water, he or she should sip some to facilitate swallowing; this also provides some lubrication. After the tube has been inserted the predetermined distance, it is checked to be sure that it is in the stomach and not in the lungs. This may be done in several ways: fluoroscopy allows visualization of the placement and is the most reliable, or gastric contents may be aspirated. ▪ INTERVENTIONS: In many hospitals a physician inserts the tube the first time; the nurse inserts it thereafter. Oral hygiene is performed regularly, and the tube, if left in place, is carefully secured with adhesive tape to the bridge of the nose. The tube is then connected to the appropriate equipment (suction, feeding tube bag, etc.), depending on the purpose for the tube and patient condition. Orders for tube feeding usually include the amount and timing of feeding, as well as the concentration and, sometimes, the ingredients of the formula. The formula is refrigerated and then warmed to room temperature. If the person is unconscious or unresponsive, suction equipment is kept at hand. An exact record of the feedings is kept. ▪ OUTCOME CRITERIA: For the patient’s comfort, the tube is selected to fit well and be suitable for the purpose of the procedure: a tight fit is irritating to the tissues, and a small tube might not allow the prescribed formula to pass through. Resistance, gagging, and wincing during tube insertion may be minimized by explaining the procedure, by a slow steady progress, and by proper lubrication of the tube and positioning of the patient.