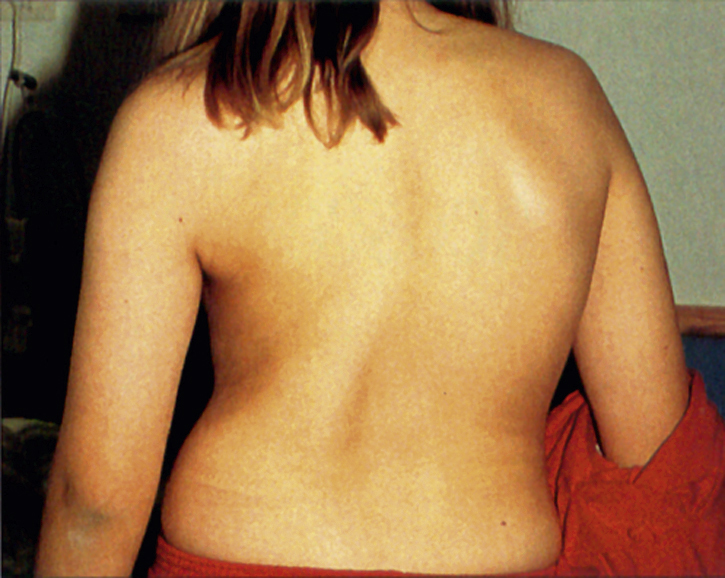
idiopathic scoliosis, an abnormal condition characterized by a lateral curvature of the spine. It is the most common type of scoliosis, evident in 70% of all patients with scoliosis and up to 80% of those with structural scoliosis. It may occur at any age, but three types are commonly associated with certain age groups. The infantile type affects 1- to 3-year-olds. The juvenile type affects 3- to 10-year-olds. The adolescent type affects preadolescents and adolescents. The main factors in diagnosing idiopathic scoliosis are the degree, balance, and rotational component of the curvature. The rotational component may contribute to rib cage deformities and impingement on the pulmonary and cardiac systems. ▪ OBSERVATIONS: The most common type is the adolescent type. Early diagnosis is difficult because the associated curvature is often hidden by clothing. Preadolescent screening is encouraged in schools. The signs commonly associated with scoliosis include unlevel shoulders, a prominent scapula, a prominent breast, a prominent flank area, an unlevel or prominent hip, poor posture, and an obvious curvature. During diagnosis it is necessary to view the patient from the front and from the back and while the patient is bending. Other signs that may be associated with idiopathic scoliosis are occasional transient pain and fatigue and decreased pulmonary function. Radiographic films of the spine in the bending position are important in ascertaining the flexibility of the curvature and the potential for spontaneous correction. Neurological deficits are commonly associated with severe curvature and vary according to the extent to which the curvature has impinged on the spinal cord. Some signs of such impingement are reflex, sensation, and motor alterations of the lower extremities. ▪ INTERVENTIONS: Nonsurgical intervention commonly uses observation, an exercise program, and a Milwaukee brace. Observation consists of frequent physical examinations and radiographic monitoring of the progress of the curvature. Exercise programs are designed to promote the maximum correction possible, as indicated by the degree of flexibility shown in the initial radiographic examination. Observation and the exercise program are used with patients who have a curvature less than 15 to 20 degrees. Greater degrees of curvature usually require the use of a Milwaukee brace in addition to observation and an exercise program. The brace, which is usually worn 23 hours a day, is used to control the progress of the curvature. The exercise program is implemented when the adolescent is out of the brace, and additional exercises are performed while in the brace. Surgical intervention may be required if the curvature has progressed to 40 degrees or more at the time of diagnosis or if a slightly lesser degree of curvature exists with a high degree of rotational component or imbalance. Approximately 5% to 10% of patients with idiopathic scoliosis require surgical intervention, which involves fusing of the involved vertebrae to prevent progress of the deformity. Preoperative traction such as Cotrel traction and halo-femoral traction may also be used to encourage gradual tissue alterations and to decrease postoperative complications. The patient may be placed in Cotrel traction for a period of 5 to 10 days before surgery. The patient may be placed in halo-femoral traction 1 to 3 weeks before surgery. Some physicians apply a preoperative cast to patients to achieve immobilization and adjustment, especially if surgery must be postponed for a considerable period after diagnosis. Common surgical intervention techniques for this condition are the Harrington rod instrumentation technique and the Dwyer cable instrumentation technique; the former is more common. Initial postoperative immobilization is achieved with a posterior plaster shell, a Milwaukee brace, or a windowed cast. A Stryker frame, Foster frame, or CircOlectric bed may also be used. Additional postoperative immobilization by means of cast therapy is often required for 8 to 12 months or until the bony union of the fused area is absolutely ensured. The usual type of cast in this application is a Risser localizer cast, applied with a degree of traction. The Risser turnbuckle cast may also be used when instrumentation has not been used. A Milwaukee brace or a plastic body jacket may be used when less immobilization is desired.