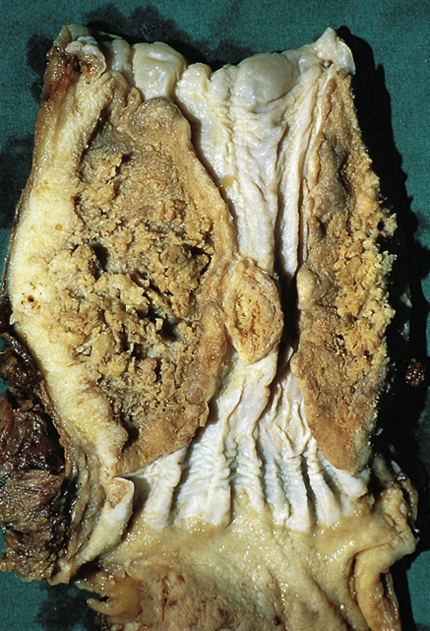
esophageal cancer, a rare malignant neoplastic disease of the esophagus that peaks at about 60 years of age, occurs three times more frequently in men than in women, and is found more often in Asia and Africa than in North America. Risk factors associated with the disease are heavy consumption of alcohol, tobacco smoking, betel-nut chewing, Plummer-Vinson syndrome, Barrett’s esophagus, and achalasia. Aflatoxin in moldy grain and peanuts or a dietary deficiency, especially of molybdenum, may be involved. See also esophagectomy. ▪ OBSERVATIONS: Esophageal cancer does not often cause any symptoms in the early stages, but in later stages produces painful dysphagia, chest pain, anorexia, weight loss, regurgitation, cervical adenopathy, and, in some cases, persistent cough. Left vocal cord paralysis and hemoptysis indicate an advanced stage of the disease. Diagnostic measures include barium swallow, fiberoptic esophagoscopy, and biopsy and cytological examination of the primary lesion and regional nodes. Most esophageal tumors are poorly differentiated squamous cell carcinomas; adenocarcinomas occur less frequently and are usually found in the lower third of the esophagus. ▪ INTERVENTIONS: Surgical treatment may require total or partial esophagectomy. Radiotherapy may eradicate early local tumors and may effectively palliate the symptoms of an advanced lesion. Chemotherapy may be used in palliation of advanced disease or as an adjuvant to surgery or radiation therapy. ▪ PATIENT CARE CONSIDERATIONS: Esophageal cancer metastasizes rapidly and thus has a poor prognosis. The tumor may spread locally to invade the trachea, bronchi, pericardium, great blood vessels, and thoracic vertebrae or may metastasize to lymph nodes, the lungs, and the liver.