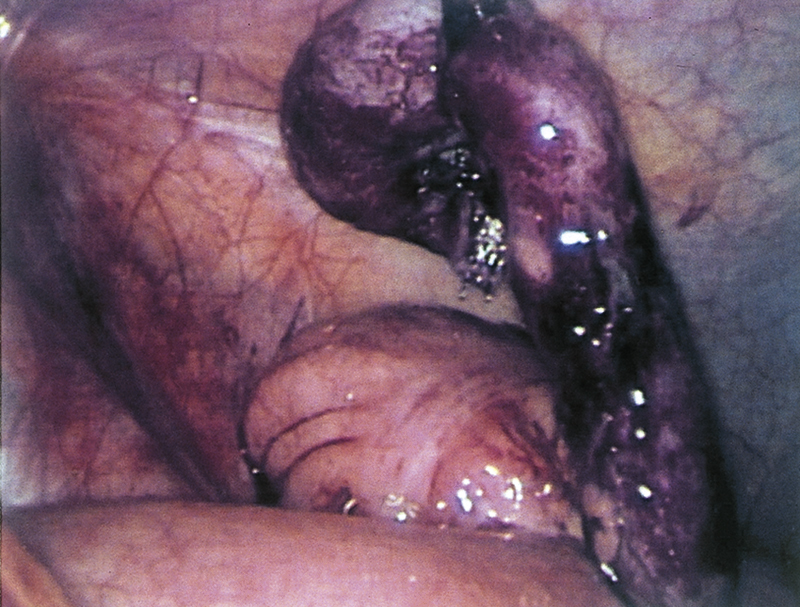
appendicitis /əpen′disī″tis/ [L, appendere + Gk, itis] , an inflammation of the vermiform appendix, usually acute, that, if undiagnosed, leads rapidly to perforation and peritonitis. The inflammation is caused by an obstruction such as a hard mass of feces or a foreign body in the lumen of the appendix, lymphoid hyperplasia, fibrous disease of the intestinal wall, an adhesion, or a parasitic infestation. Appendicitis is most likely to occur in teenagers and young adults and is more prevalent in male patients. Kinds include chronic appendicitis.  OBSERVATIONS: The most common symptom is constant pain in the right lower quadrant of the abdomen around McBurney’s point, which the patient describes as having begun as intermittent pain in midabdomen. Rebound tenderness occurs at McBurney’s point as well. Pain may also occur on the left side. Extreme tenderness occurs over the right rectus abdominis muscle. To decrease the pain, the patient keeps the knees bent to prevent tension of the abdominal muscles. Appendicitis is characterized by vomiting, a low-grade fever of 99° to 102° F, an elevated white blood cell count, rebound tenderness, a rigid abdomen, and decreased or absent bowel sounds. Other indications of peritonitis include increasing abdominal distension, acute abdomen, tachycardia, rapid and shallow breathing, and restlessness. If peritonitis is suspected, IV antibiotic therapy, fluids, and electrolytes are given. PATIENT CARE CONSIDERATIONS: The nurse is alert to the signs and symptoms of rupture and peritonitis and provides education about the diagnosis, treatment, and recovery. PATIENT CARE CONSIDERATIONS: Treatment is appendectomy within 24 to 48 hours of the first symptoms because delay usually results in rupture and peritonitis as fecal matter is released into the peritoneal cavity. The fever rises sharply once peritonitis begins. The patient may have sudden relief from pain immediately after rupture, followed by increased, diffuse pain.
OBSERVATIONS: The most common symptom is constant pain in the right lower quadrant of the abdomen around McBurney’s point, which the patient describes as having begun as intermittent pain in midabdomen. Rebound tenderness occurs at McBurney’s point as well. Pain may also occur on the left side. Extreme tenderness occurs over the right rectus abdominis muscle. To decrease the pain, the patient keeps the knees bent to prevent tension of the abdominal muscles. Appendicitis is characterized by vomiting, a low-grade fever of 99° to 102° F, an elevated white blood cell count, rebound tenderness, a rigid abdomen, and decreased or absent bowel sounds. Other indications of peritonitis include increasing abdominal distension, acute abdomen, tachycardia, rapid and shallow breathing, and restlessness. If peritonitis is suspected, IV antibiotic therapy, fluids, and electrolytes are given. PATIENT CARE CONSIDERATIONS: The nurse is alert to the signs and symptoms of rupture and peritonitis and provides education about the diagnosis, treatment, and recovery. PATIENT CARE CONSIDERATIONS: Treatment is appendectomy within 24 to 48 hours of the first symptoms because delay usually results in rupture and peritonitis as fecal matter is released into the peritoneal cavity. The fever rises sharply once peritonitis begins. The patient may have sudden relief from pain immediately after rupture, followed by increased, diffuse pain.