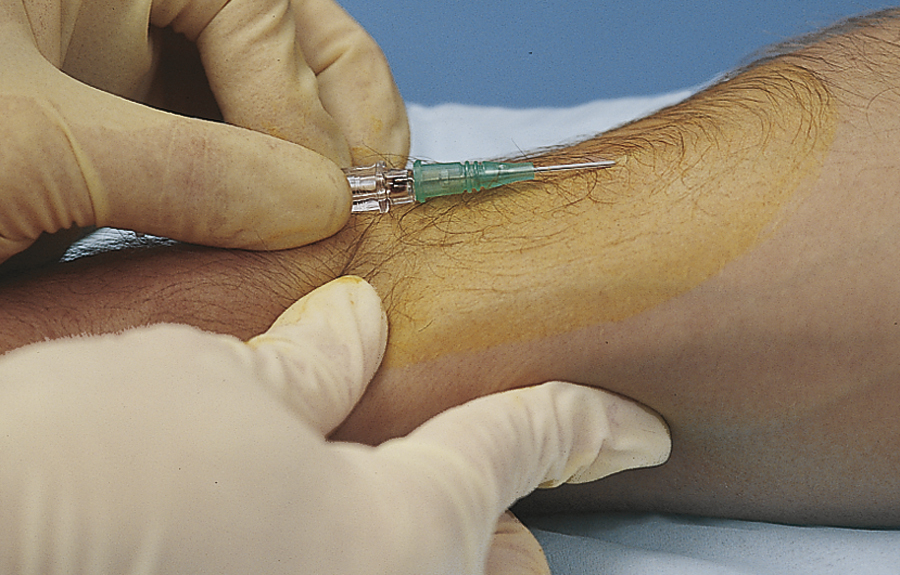
venipuncture /ven′əpungk″chər/ [L, vena + pungere, to prick] , the transcutaneous puncture of a vein by a sharp rigid stylet or cannula carrying a flexible plastic catheter or by a steel needle attached to a syringe or catheter. It is done to withdraw a specimen of blood, perform a phlebotomy, instill a medication, start an IV infusion, or inject a radiopaque substance for radiological examination of a part or system of the body. Also spelled venepuncture. See also phlebotomy, intravenous infusion. ▪ METHOD: The specific steps in performing a venipuncture vary with the purpose of the procedure and the equipment to be used, but in most instances it begins as follows: The nurse dons disposable gloves. A convenient vein is selected, usually on the outside of the forearm, on the back of the hand, or in the antecubital fossa. The vein is palpated, and to dilate the vein a tourniquet is wrapped around the arm proximal to the intended site of puncture. After cleansing the intended insertion site, the examiner avoids touching the site with the gloved finger(s). The vein is immobilized by applying traction on the skin around the puncture site. The stylet or needle is held at an angle of 30 degrees for direct venipuncture. In performing direct venipuncture, the tip of the needle is pointed in the direction of the flow of blood and advanced through the skin directly into the vein. The tip is usually inserted bevel side up; however, if a large-bore needle must be used in a small vein, it is preferable to insert the needle bevel side down because it is less likely to perforate the posterior wall of the vein. After the skin is punctured, little resistance is felt as the tip passes through the subcutaneous tissue, but a sudden slight resistance may be felt as the tip hits the wall of the vein. At this point the tip is cautiously advanced, with the needle or stylet held nearly flush with the skin. Slight upward pressure aids in keeping the tip in the vein as it is advanced into the lumen of the IV space. Blood flows back into the hub of the needle or into the catheter attached to the needle or covering the stylet, and the tip of the needle usually can be felt to be in the vein. If these signs are absent, the tip is not in the vein, in which case it is usually best to remove the needle or stylet, apply pressure to the puncture site, and start the procedure again, using new equipment. ▪ INTERVENTIONS: Wing-tipped “butterfly” needles, various kinds of intracatheters, and single or multiple venipuncture needles require familiarity and practice for correct insertion and stabilization. A sterile dressing and an antimicrobial ointment are applied over the insertion site. The cleansing agent used to prepare the injection site may be iodine, povidone-iodine, or ethyl alcohol. If an iodine preparation or solution is to be used, the patient is first asked about any previous allergic reaction to iodine. To aid insertion of the tip into the vein, the patient may be asked to clench the fist to further dilate the vein. The use of the gloves helps to protect the health care worker from inadvertent contact with the patient’s blood. ▪ OUTCOME CRITERIA: Aseptic technique is required to avoid infection. A quick, skillful insertion is nearly painless for the patient. Specific sequelae to venipuncture vary with the techniques and equipment used.