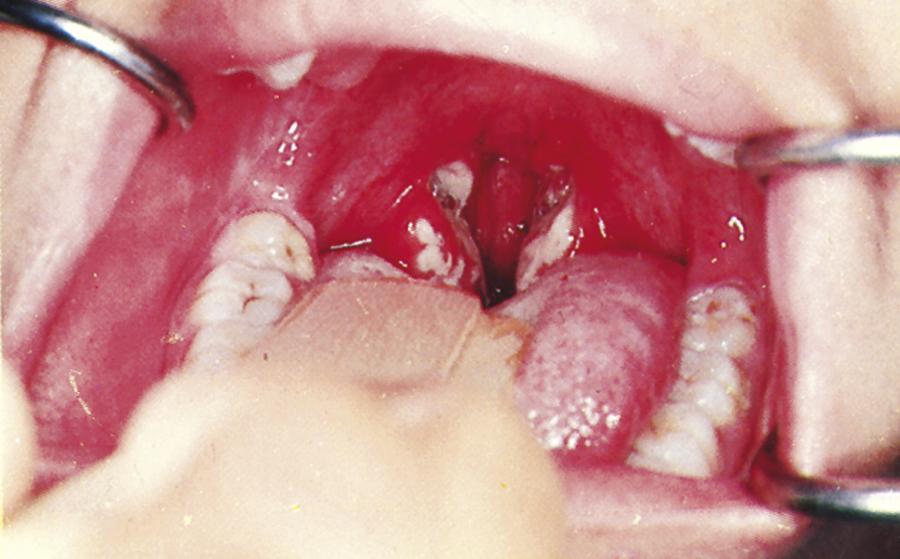
tonsillitis /-ī′tis/ , an infection or inflammation of a tonsil. Acute tonsillitis, frequently caused by Streptococcus infection, is characterized by severe sore throat, fever, headache, malaise, difficulty in swallowing, earache, and enlarged tender lymph nodes in the neck. Acute tonsillitis may accompany scarlet fever. Treatment includes systemic antibiotics, analgesics, and warm irrigations of the throat. Soft foods and ample fluids are given. Tonsillectomy is sometimes performed for recurrent tonsillitis or tonsillar abscess. See also acute tonsillitis, peritonsillar abscess, scarlet fever, strep throat.  OBSERVATIONS: Symptoms include a moderate to severe sore throat, lasting longer than 2 days; difficulty swallowing; pain referred to the ears; enlarged anterior cervical nodes; fever and chills; headache; muscle and joint pain; anorexia; increased secretions from the throat; enlarged, reddened, inflamed tonsils; pus or exudate on the tonsils; halitosis; and edematous or inflamed uvula. Symptoms often last 2 to 3 days after treatment is initiated. Diagnosis is made by direct inspection of the throat and tonsils, and throat cultures are used to identify the causative organism. If not treated, the following can occur: peritonsillar abscess, airway occlusion, rheumatic fever and subsequent cardiovascular disorders, kidney failure, or poststreptococcal glomerulonephritis. INTERVENTIONS: Treatment is directed at the symptoms. Antibiotics are given if the cause is bacterial. Analgesics are used for pain relief. Tonsillectomy is indicated for massive hypertrophy that restricts breathing or obstructs the airway. Adenoidectomy is indicated for hypertrophy of adenoids that obstruct nasal breathing. PATIENT CARE CONSIDERATIONS: Nursing care is focused on provision of comfort and rest. Warm, bland fluids or very cold fluids, saltwater gargles, and throat lozenges may alleviate throat discomfort. A cool mist vaporizer and adequate fluids keep mucous membranes moist. Postsurgical care is aimed at prevention of hemorrhage, prevention of aspiration of drainage, and control of pain. The child is positioned on side until fully alert to facilitate drainage of secretions and prevent aspiration. Suctioning is done with care to prevent trauma to the oropharynx. Frequent assessment for bleeding is done with direct visualization of the surgical site. Continual swallowing by child is an obvious sign of early bleeding. Coughing, clearing of throat, and nose blowing are discouraged and activity is limited to prevent hemorrhage. An ice collar may be applied to help alleviate discomfort from sore throat. Continuous pain control and mild sedation is necessary to prevent crying, which can irritate the operative site and promote hemorrhage. Parents should be educated about signs of hemorrhage and prevention (limiting activity, discouraging coughing, clearing throat, avoiding throat irritants, gargles). Instruction is given to treat any sign of bleeding as a medical emergency.
OBSERVATIONS: Symptoms include a moderate to severe sore throat, lasting longer than 2 days; difficulty swallowing; pain referred to the ears; enlarged anterior cervical nodes; fever and chills; headache; muscle and joint pain; anorexia; increased secretions from the throat; enlarged, reddened, inflamed tonsils; pus or exudate on the tonsils; halitosis; and edematous or inflamed uvula. Symptoms often last 2 to 3 days after treatment is initiated. Diagnosis is made by direct inspection of the throat and tonsils, and throat cultures are used to identify the causative organism. If not treated, the following can occur: peritonsillar abscess, airway occlusion, rheumatic fever and subsequent cardiovascular disorders, kidney failure, or poststreptococcal glomerulonephritis. INTERVENTIONS: Treatment is directed at the symptoms. Antibiotics are given if the cause is bacterial. Analgesics are used for pain relief. Tonsillectomy is indicated for massive hypertrophy that restricts breathing or obstructs the airway. Adenoidectomy is indicated for hypertrophy of adenoids that obstruct nasal breathing. PATIENT CARE CONSIDERATIONS: Nursing care is focused on provision of comfort and rest. Warm, bland fluids or very cold fluids, saltwater gargles, and throat lozenges may alleviate throat discomfort. A cool mist vaporizer and adequate fluids keep mucous membranes moist. Postsurgical care is aimed at prevention of hemorrhage, prevention of aspiration of drainage, and control of pain. The child is positioned on side until fully alert to facilitate drainage of secretions and prevent aspiration. Suctioning is done with care to prevent trauma to the oropharynx. Frequent assessment for bleeding is done with direct visualization of the surgical site. Continual swallowing by child is an obvious sign of early bleeding. Coughing, clearing of throat, and nose blowing are discouraged and activity is limited to prevent hemorrhage. An ice collar may be applied to help alleviate discomfort from sore throat. Continuous pain control and mild sedation is necessary to prevent crying, which can irritate the operative site and promote hemorrhage. Parents should be educated about signs of hemorrhage and prevention (limiting activity, discouraging coughing, clearing throat, avoiding throat irritants, gargles). Instruction is given to treat any sign of bleeding as a medical emergency.