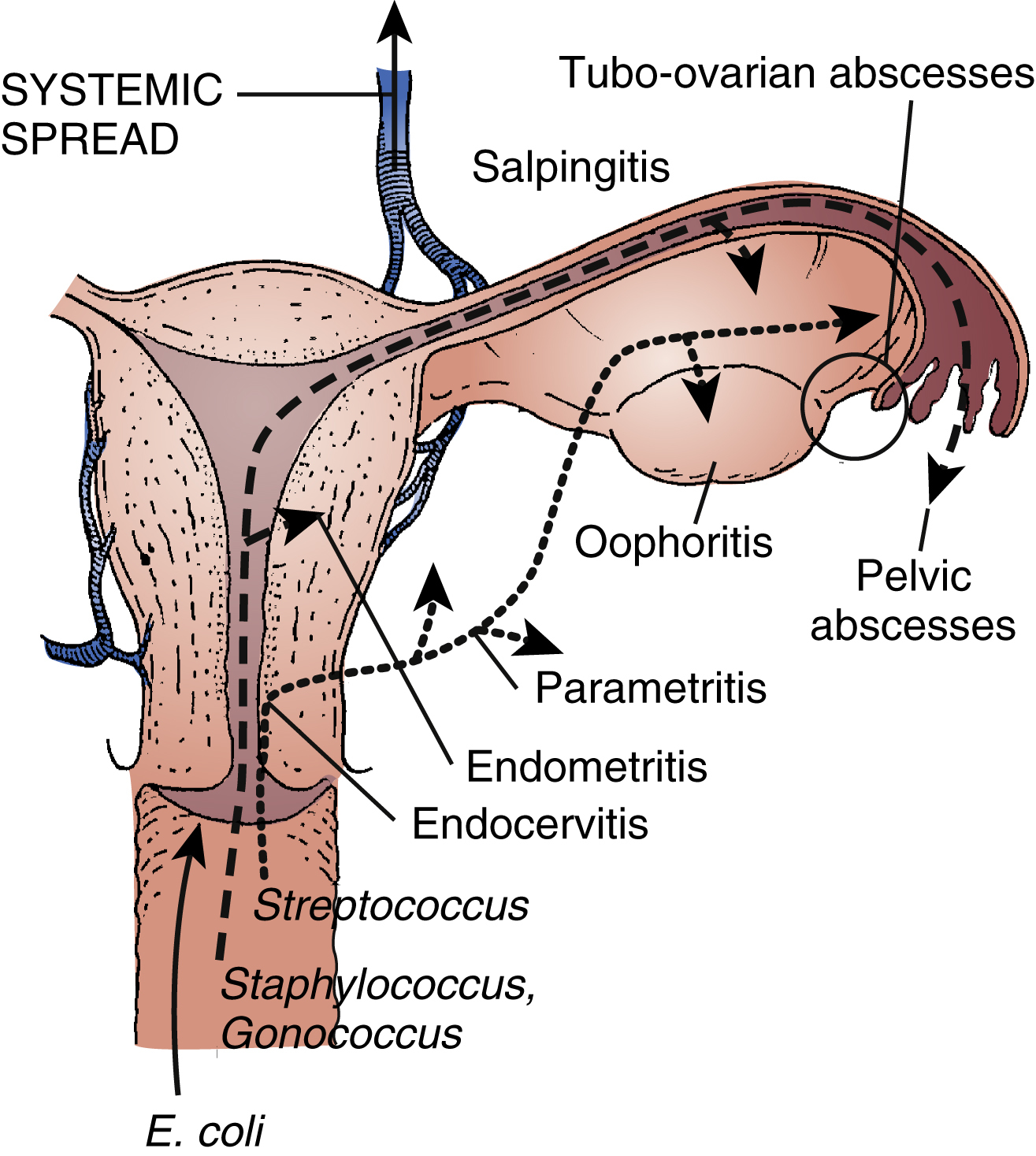
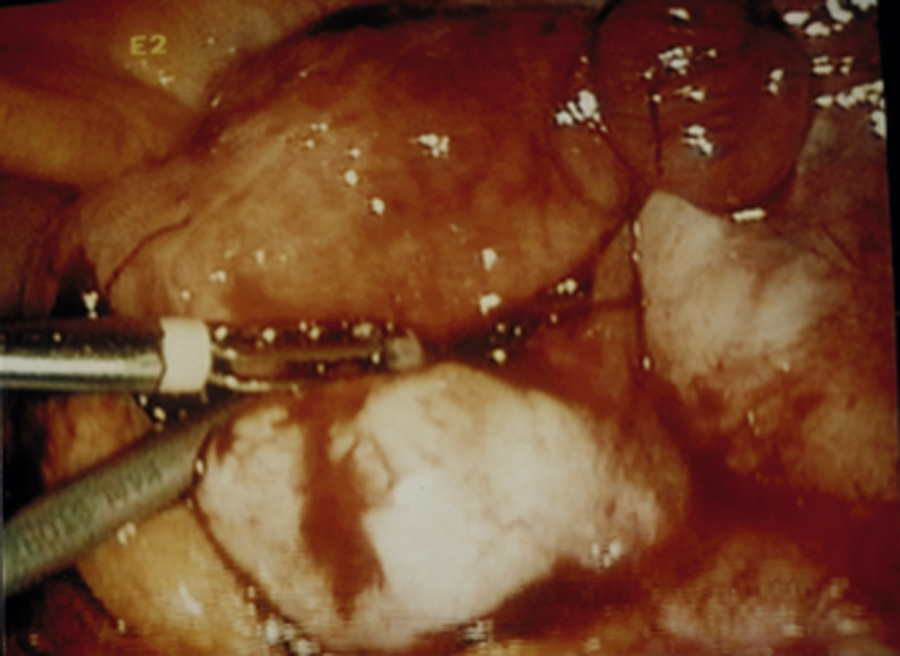
pelvic inflammatory disease (PID), any inflammatory condition of the female pelvic organs, especially one caused by bacterial infection. Characteristics of the condition include fever; foul-smelling vaginal discharge; pain in the lower abdomen; abnormal uterine bleeding; pain with coitus; and tenderness or pain in the uterus, affected ovary, or fallopian tube on bimanual pelvic examination. If an abscess has already developed, a soft, tender fluid-filled mass may be palpated. Bed rest and antibiotics are usually prescribed, but surgical drainage of an abscess may be required. Severe, fulminating PID may necessitate hysterectomy to prevent fatal septicemia. If the cause is infection by gonococci or chlamydiae, the woman’s sexual partners are also treated with antibiotics. Severe PID is usually very painful. The woman may be prostrate and require narcotic analgesia. Recurrent or severe PID often results in scarring of the fallopian tubes, obstruction, and infertility. ▪ OBSERVATIONS: PID may be either acute or chronic. Acute onset typically occurs after onset of menses. Symptoms typically include progressive lower abdominal pain with guarding and rebound tenderness, fever, copious purulent cervical discharge, nausea and vomiting, malaise, urinary urgency and frequency, vaginal itching, and maceration. Chronic PID is manifested as chronic pain, menstrual irregularities, and recurrence and exacerbation of acute symptoms. Diagnosis is made through a clinical exam that reveals typical symptomatology coupled with elevated WBCs and erythrocyte sedimentation rate plus a positive culture of secretions. On pelvic examination, moving of the cervix causes severe pain and rebound tenderness that is present in the abdomen. Transvaginal ultrasound may show thickened fluid-filled fallopian tubes or adnexal mass. MRI and laparoscopy may be used to detect pelvic abnormalities. Common complications include general peritonitis, sterility, and ectopic pregnancy. ▪ INTERVENTIONS: Acute treatment is aimed at control and alleviation of infection with combinations of antiinfective drugs. Laparoscopy may be used to drain antibiotic-resistant abscesses, salpingolysis to remove adhesions, salpingostomy to reopen blocked fallopian tubes, and salpingo-oophorectomy for ruptured fallopian tubes or ectopic pregnancy. In vitro fertilization may be used in women with PID-induced sterility who wish to have children. ▪ PATIENT CARE CONSIDERATIONS: Nursing plays a key role in prevention, early recognition, and prompt treatment. Education is aimed at reducing factors that place women at increased risk, such as unprotected sex, multiple sex partners, exposure to urethritis, or STDs, and frequent vaginal douching; recognizing conditions that make one more susceptible to PID, such as IUD insertion, recent abortion, or pelvic surgery, and improper use of antibiotics; and seeking treatment for any signs of vaginal infection, such as any evidence of abnormal vaginal odor or discharge. Acute care is supportive and aimed at adequate rest in a semi-Fowler’s position and adequate hydration. IUDs require removal during treatment. Instruction is given about the proper use of antibiotics. Education stresses sexual abstinence and avoidance of tampons and douching during treatment. Sexual partners need to be tracked and treated if PID was associated with an STD.