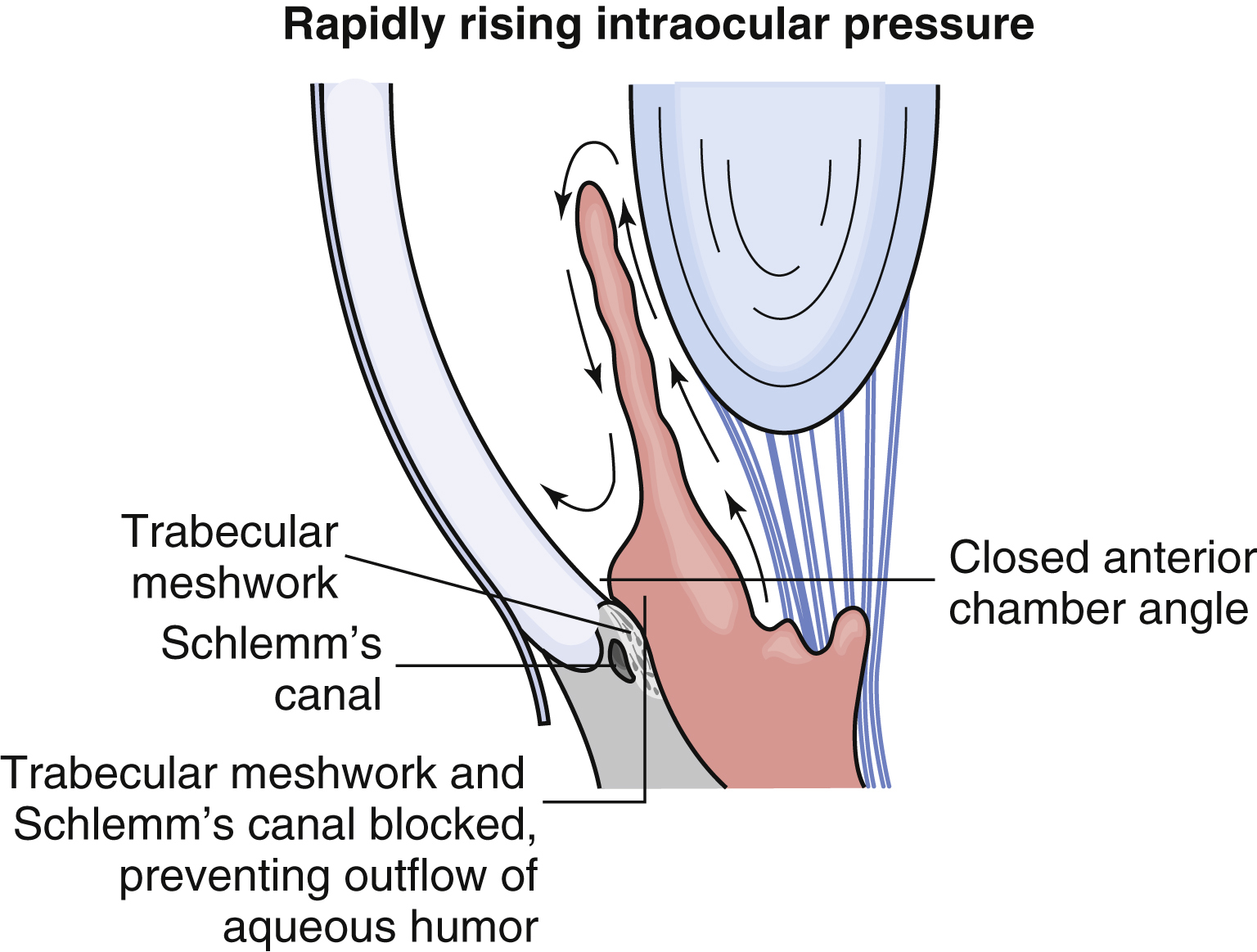
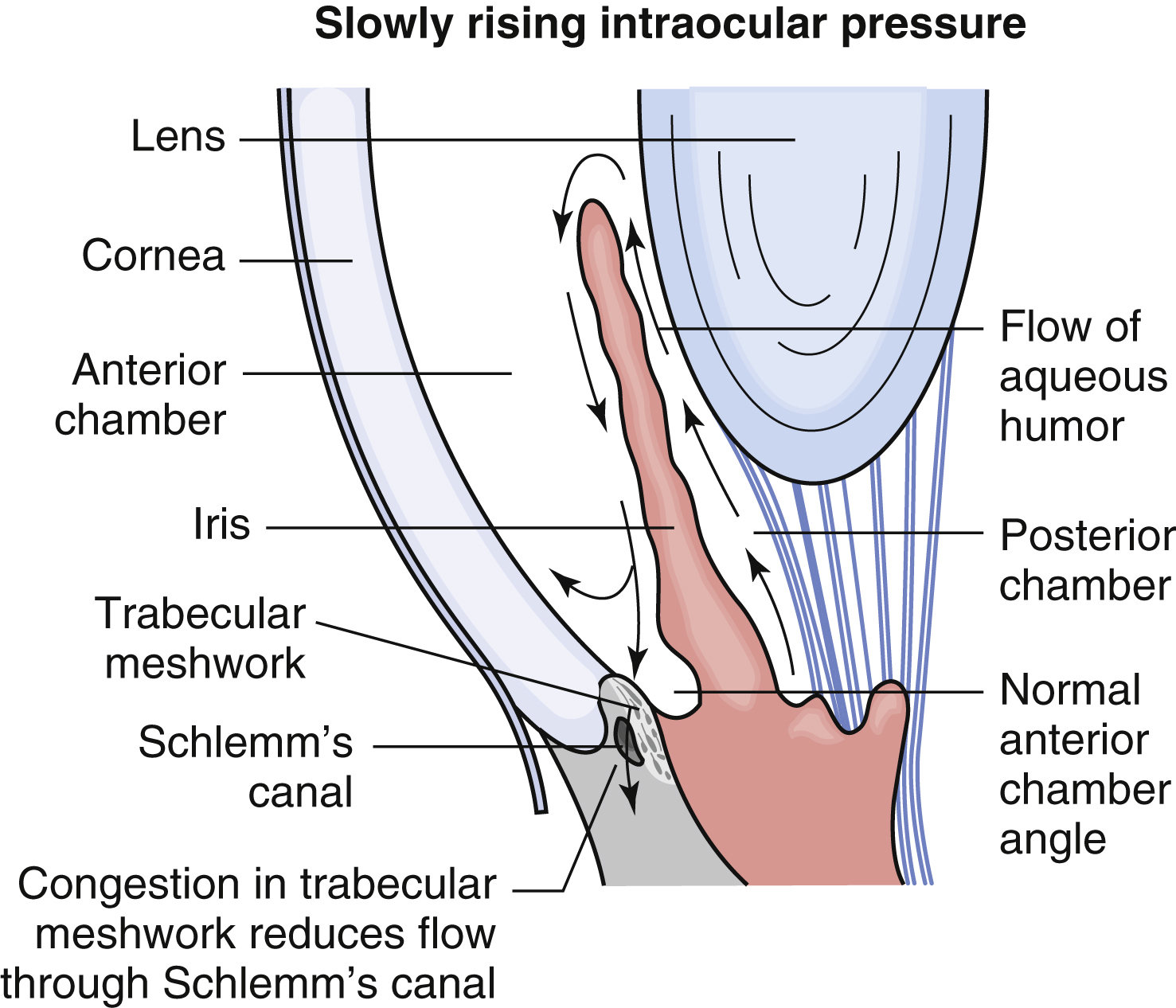
glaucoma /glôkō″mə, glou-/ [Gk, cataract] , an abnormal condition of elevated pressure within an eye that occurs when aqueous production exceeds aqueous outflow, resulting in damage to the optic nerve. Acute (angle-closure, closed-angle, or narrow-angle) glaucoma occurs if the pupil in an eye with a narrow angle between the iris and cornea dilates markedly, causing obstruction of aqueous humor drainage from the anterior chamber. Primary open-angle glaucoma (POAG) is much more common in the United States and develops slowly and insidiously without a narrow angle. Peripheral visual field losses are most common, developing often without the patient’s awareness until there is very serious disease. The obstruction is believed to occur within the trabecular meshworks. −glaucomatous, adj. ▪ OBSERVATIONS: Acute angle-closure glaucoma is accompanied by extreme ocular pain, blurred vision, redness of the eye, and dilation of the pupil. Nausea and vomiting may occur. If untreated, acute glaucoma causes complete and permanent blindness within 2 to 5 days. Chronic open-angle glaucoma may produce no symptoms except gradual loss of peripheral vision over a period of years. Sometimes present are headaches, blurred vision, and dull pain in the eye. Cupping of the optic discs may be noted on ophthalmoscopic examination. Halos around lights and central blindness are late manifestations. Both types are characterized by elevated intraocular pressure indicated by tonometry. ▪ INTERVENTIONS: Acute glaucoma is treated with eyedrops to constrict the pupil and draw the iris away from the cornea; osmotic agents such as mannitol or glycerol given systemically to lower intraocular pressure; acetazolamide to reduce fluid formation; and surgical iridectomy to produce a filtration pathway for aqueous humor. Chronic glaucoma can usually be controlled with eyedrops such as beta-blockers, alpha-agonists, topical carbonic anhydrase inhibitors, and prostaglandin analogs.